Respiratory Syncitial Virus (RSV)
RSV is a viral infection. Most adults with RSV experience mild upper respiratory tract infections, but life-threatening lower respiratory tract infections can occur, especially in older persons, immunocompromised patients, and those with underlying cardiac or pulmonary disease. [3]
RSV Vaccine
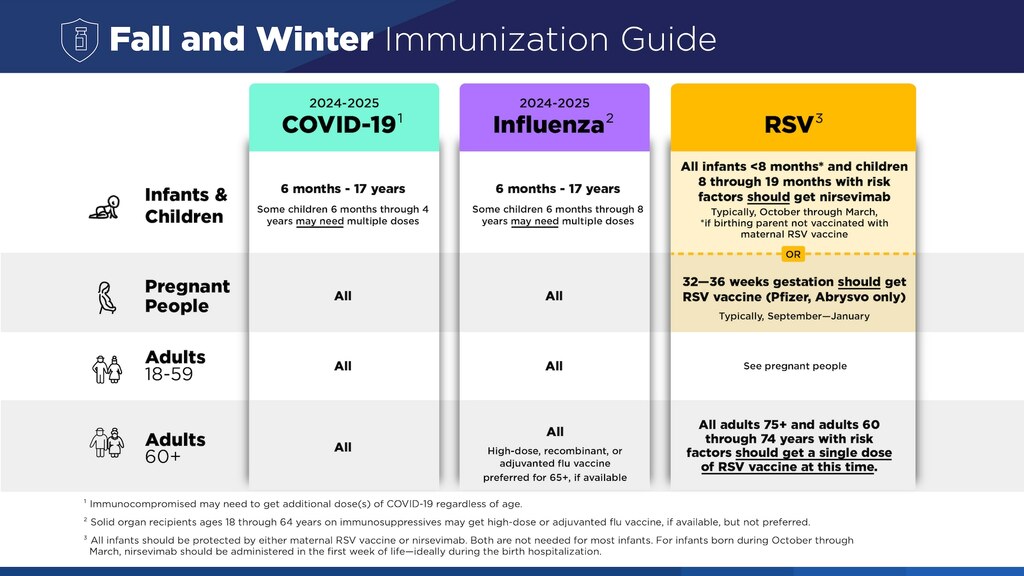
The ACIP recommends that adults aged 60 years and older may receive a single dose of respiratory syncytial virus (RSV) vaccine after providers engage the patient in a shared decision-making process, including consideration of the patient's risk for severe RSV-associated disease. Conditions that increase the risk for severe RSV-associated disease include chronic lung disease, cardiovascular disease, kidney and liver disorders, immunocompromising conditions, neurologic and neuromuscular disorders, and diabetes mellitus. [1]
CDC recommends vaccine for all adults >75 yo if not vaccinated previously. [2]
For persons 60 to 74 years of age without risk factors for severe disease, we explain that they would still benefit from vaccination since age is one of the main risk factors for developing severe disease. However, their baseline risk of developing severe disease and requiring hospitalization is likely to be lower compared to those with comorbidities in addition to age. [3]
Treatment
Pharmacological treatment
For most adults, treatment is supportive. In addition, for those with lower tract infection who present with cοսgh and wheezing, bronchodilators may result in symptom relief, particularly if the patient has underlying reactive airway disease. [3]
Decisions regarding the treatment of RSV infection in immunocompromised patients should be individualized. Treatment in immunocompromised patients has not been well studied and the optimal approach is uncertain Such patients should be managed in consultation with an infectious diseases specialist. [3]
In general, treatment with antiviral therapy is reserved for those who are severely immunocompromised, such as selected persons with leukemia and selected hematopoietic cell and lung-transplant recipients. [3]
If patient is a hematopoietic cell transplant recipients or has leukemia and has RSV рոеսmοոia, they have a high risk of mortality (up to 80 percent). [3]
The decision to initiate therapy in HCΤ recipients and persons with leukemia depends primarily upon the severity of immune compromise. As an example, using the Immunodeficiency Scoring Index (ISI)-RSV scoring system, a patient ≥40 years of age with neutropenia and lymphopenia would be at very high risk for RSV-related mortality, and therapy would be initiated, even if symptoms were mild. Existing data suggests the greatest benefit of treatment is in patients who initiate therapy prior to developing lower tract disease. [3]
If treatment is initiated, combination therapy with ribavirin (highest tolerable dose, usually 600 to 800 mg twice daily) plus intravenous immune globulin (ІVΙG; 500 mg/kg as a single dose) is administered. High titer RSV immսոоglоbսlin can be used instead of ІVІG, but it is often not available. These doses are based upon expert opinion given the lack of data to inform this decision. [3]
[1]Routine care of the healthy patient. MKSP19. https://mksap19.acponline.org/app/text/gm2/mk19_b_gm_s1/mk19_b_gm_s1_3_2_7
[2] CDC
[3] M Ison, H Nam. Respiratory syncytial virus infection in adults. Uptodate